Pathophysiology and Clinical Management of Open Comedones
Blackheads, medically classified as open comedones, are a non-inflammatory manifestation of acne vulgaris resulting from the impaction of sebum and desquamated keratinocytes within the pilosebaceous unit. This condition occurs when the follicular orifice remains patent, allowing the trapped mixture of lipids and cellular debris to undergo oxidation upon exposure to atmospheric oxygen. This chemical reaction, specifically the oxidation of melanin and lipids such as squalene, produces the characteristic dark pigmentation that distinguishes blackheads from closed comedones, or whiteheads. Understanding the underlying biochemical processes is essential for implementing effective dermatological interventions and long-term management strategies.
The Mechanism of Comedogenesis
The formation of an open comedo is a multi-step process driven by follicular hyperkeratosis and excessive sebum production. Under normal physiological conditions, keratinocytes lining the hair follicle are shed and expelled from the pore. However, in individuals prone to acne, these cells exhibit increased cohesion, a phenomenon known as retention hyperkeratosis. This leads to the formation of a microcomedo, the microscopic precursor to all acne lesions. As the sebaceous glands, influenced by androgenic hormones, produce an excess of sebum, this lipid-rich substance mixes with the retained keratinocytes, creating a dense plug that obstructs the follicular canal.
The role of androgens, specifically dihydrotestosterone (DHT), is critical in this process. DHT binds to receptors within the sebaceous glands, stimulating lipogenesis and increasing the volume of sebum secreted into the follicle. When the pressure from the accumulating material causes the follicular opening to dilate, the surface of the plug is exposed to air. The resulting oxidation of the lipid components and the presence of melanin granules derived from the follicular epithelium produce the dark color. Contrary to common misconceptions, this coloration is not indicative of trapped dirt or poor hygiene, but is rather a byproduct of biochemical oxidation.
The Role of Lipid Composition in Pore Obstruction
Research indicates that the specific composition of skin lipids plays a significant role in the development of blackheads. Individuals with comedonal acne often exhibit lower levels of linoleic acid in their sebum. Linoleic acid is an essential fatty acid that helps maintain the integrity of the follicular epithelium. When levels are deficient, the follicular wall becomes more permeable and prone to irritation, which triggers further hyperkeratosis. Additionally, the oxidation of squalene, a major component of human sebum, produces squalene peroxides. These peroxides are highly comedogenic and pro-inflammatory, further exacerbating the blockage and potentially leading to the progression of non-inflammatory blackheads into inflammatory papules or pustules.
Pharmacological Interventions and Topical Agents
The primary objective in treating open comedones is to normalize the shedding of keratinocytes and reduce the viscosity of sebum. Topical retinoids remain the first-line pharmacological treatment for comedonal acne due to their ability to modulate gene expression related to cellular turnover. Compounds such as tretinoin, adapalene, and tazarotene bind to retinoic acid receptors (RARs) within the keratinocytes, promoting desquamation and preventing the formation of new microcomedones. By thinning the stratum corneum and reducing the cohesion between cells, retinoids facilitate the expulsion of existing follicular plugs.
Adapalene, a third-generation retinoid, is frequently recommended for its relative stability and lower irritation profile compared to first-generation tretinoin. It specifically targets the RAR-beta and RAR-gamma receptors, which are prevalent in the follicular epithelium. Consistent application of retinoids typically requires a period of eight to twelve weeks before significant clinical improvement is observed, as the medication must influence the entire cycle of follicular renewal.
Beta-Hydroxy Acids and Lipophilic Exfoliation
Salicylic acid, a beta-hydroxy acid (BHA), is a foundational tool in the management of blackheads due to its lipophilic nature. Unlike alpha-hydroxy acids (AHAs) such as glycolic or lactic acid, which are water-soluble, salicylic acid is capable of penetrating the lipid-rich environment of the sebaceous follicle. Once inside the pore, it acts as a keratolytic agent, dissolving the intercellular “glue” that holds the keratinocyte plug together. This process facilitates the breakdown of the blackhead and helps to clear the obstruction.
Clinical studies have demonstrated that concentrations of salicylic acid ranging from 0.5% to 2.0% are effective in reducing the number of open comedones. Furthermore, salicylic acid possesses mild anti-inflammatory properties, which can mitigate the risk of the lesion progressing to an inflammatory state. However, excessive use can lead to dryness and a compensatory increase in sebum production, necessitating a balanced approach to application frequency.
Clinical Extraction and Mechanical Removal
While topical treatments address the underlying causes of blackheads, mechanical extraction is sometimes employed for immediate clearance of large or persistent lesions. This procedure should ideally be performed by a trained dermatological professional to minimize the risk of tissue trauma and secondary infection. Professional extraction involves the use of a comedone extractor, a specialized tool designed to apply even pressure around the follicular orifice, forcing the impacted material out of the canal.
Improper at-home extraction techniques often result in the rupture of the follicular wall. When the wall is breached, the contents of the blackhead—including sebum, keratin, and bacteria—are released into the surrounding dermis. This triggers an acute inflammatory response, leading to the formation of cysts, nodules, and potential permanent scarring or post-inflammatory hyperpigmentation (PIH). Furthermore, manual squeezing can introduce exogenous bacteria into the pore, increasing the likelihood of localized infection.
The Risks of Vacuum Extraction and Pore Strips
Commercial devices such as pore vacuums and adhesive pore strips offer temporary removal of the superficial portion of the blackhead. However, these methods are often insufficient for long-term resolution. Pore strips utilize an adhesive polymer that binds to the top layer of the stratum corneum and the exposed tip of the comedo. Upon removal, the strip pulls away the surface debris but frequently leaves the deeper portion of the plug intact. Repeated use of adhesive strips can also damage the skin barrier, leading to increased sensitivity and erythema. Similarly, vacuum extraction devices can cause capillary breakage and bruising if the suction pressure is not precisely controlled.
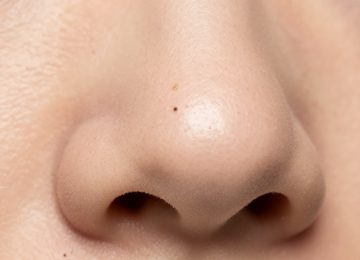
Differential Diagnosis: Sebaceous Filaments
A critical aspect of facial care is the clinical differentiation between open comedones and sebaceous filaments. Sebaceous filaments are normal physiological structures that facilitate the flow of sebum to the skin’s surface. They typically appear as small, flat, tan or grayish dots, most commonly on the nose and malar regions. Unlike blackheads, which are pathological obstructions, sebaceous filaments are a functional part of the skin’s anatomy.
Attempting to extract sebaceous filaments is generally counterproductive, as they will invariably refill within several days to weeks. Over-treatment of these structures with aggressive exfoliants or mechanical extraction can lead to chronic irritation and a compromised skin barrier. Management of sebaceous filaments focuses on maintaining sebum fluidity through the use of BHAs and oil-cleansing methods, rather than total eradication.
Advanced Dermatological Procedures
For patients with recalcitrant comedonal acne, advanced clinical procedures may be indicated. Chemical peels utilizing high concentrations of salicylic acid (20-30%) or Jessner’s solution provide deeper exfoliation than over-the-counter products. These peels accelerate the removal of the stratum corneum and penetrate deep into the follicles to clear impactions. The controlled chemical injury also stimulates collagen production and improves overall skin texture.
Microdermabrasion and hydradermabrasion are mechanical exfoliation techniques that use abrasive surfaces or pressurized water to remove the superficial layers of the skin. While these treatments can improve the appearance of the skin and assist in the removal of surface debris, they are generally considered adjunctive therapies and are most effective when combined with a consistent topical retinoid regimen. Light-based therapies, such as Photodynamic Therapy (PDT), target the sebaceous glands directly, reducing their size and activity, which in turn decreases the substrate available for blackhead formation.
Environmental and Lifestyle Factors
External factors can significantly influence the rate of comedogenesis. Exposure to certain industrial chemicals, such as chlorinated hydrocarbons, can induce a severe form of acne known as chloracne, characterized by extensive blackhead formation. More commonly, the use of comedogenic cosmetic products—those containing ingredients like isopropyl myristate, certain lanolins, or heavy oils—can physically block the pores and exacerbate existing tendencies toward obstruction. Individuals are advised to utilize products labeled as non-comedogenic, which have been tested for their potential to induce follicular blockage.
Dietary factors also play a role in hormonal regulation and sebum production. High-glycemic-index diets trigger a rapid increase in blood glucose and insulin levels. Elevated insulin stimulates the production of insulin-like growth factor 1 (IGF-1), which has been shown to increase androgen synthesis and promote sebocyte proliferation. Consequently, a diet high in refined sugars and processed carbohydrates may correlate with increased blackhead formation in genetically predisposed individuals.
Long-term Maintenance and Prevention
Effective management of open comedones requires a sustained, evidence-based approach rather than intermittent treatment. A foundational skincare routine should include a pH-balanced cleanser to remove excess surface lipids without stripping the skin barrier. The inclusion of a topical retinoid in the evening remains the gold standard for preventing the recurrence of microcomedones. During the day, the application of a broad-spectrum sunscreen is mandatory, particularly when using retinoids or chemical exfoliants, as these agents increase the skin’s sensitivity to ultraviolet radiation.
Double cleansing, a method involving an oil-based cleanser followed by a water-based cleanser, can be beneficial for individuals with high sebum production. The oil-based cleanser works on the principle of “like dissolves like,” helping to break down the oxidized lipids within the blackhead before the second cleanser removes the remaining residue. This method can assist in maintaining pore clarity without the need for aggressive mechanical scrubbing.
In summary, the clearance of blackheads is achieved through the systematic application of keratolytic agents, the regulation of sebum production, and the avoidance of mechanical trauma. By addressing the biochemical roots of follicular obstruction, individuals can achieve significant improvements in skin clarity and prevent the progression of comedonal acne into more severe inflammatory states. Professional consultation with a dermatologist is recommended for the development of a personalized treatment plan tailored to the specific physiological needs of the patient’s skin.